Diaphragmatic breathing and hiatal hernia
In clinical practice, hiatal hernia is commonly managed with proton pump inhibitors and dietary measures. These interventions have a clear role and are often necessary to control symptoms. However, there is a physiological aspect that receives far less attention in routine management: the mechanical and neurological role of the diaphragm.
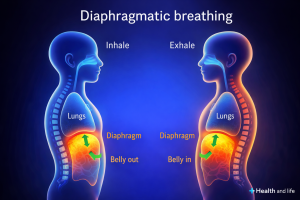
The diaphragm is not simply a respiratory muscle. It forms the anatomical boundary between the thoracic and abdominal cavities. It participates in the regulation of intra‑abdominal pressure and maintains a direct relationship with the vagus nerve and with the balance of the autonomic nervous system.
In many patients with hiatal hernia, an altered breathing pattern can be observed that has often been present for years. Breathing tends to be shallow, rapid and predominantly thoracic. This pattern maintains persistent tension in the crural diaphragm, increases the gastro‑esophageal pressure gradient and contributes to a state of low‑grade sympathetic activation. In this context, reflux, pain and visceral hypersensitivity tend to persist.
Slow diaphragmatic breathing can interrupt this cycle at several physiological levels simultaneously. It promotes a more appropriate distribution of intra‑abdominal pressure, stimulates the vagus nerve through mechanical and baroreceptor pathways and facilitates a shift toward parasympathetic predominance. It is in this state that digestive processes function more efficiently, inflammatory responses are better regulated and pain perception tends to decrease.
An aspect that recent research has begun to explore in greater depth is the concept of interoceptive dysregulation in chronic visceral disorders. In a proportion of patients with hiatal hernia there is a genuine difficulty in identifying and interpreting internal bodily signals. Structured breathing practice does not act only on respiratory mechanics. It progressively retrains internal bodily perception, a factor that several studies associate with a reduction in symptoms and an improvement in quality of life.
For this reason, in my clinical practice I usually recommend a simple routine: five minutes of slow diaphragmatic breathing before meals and during moments of stress.
The capacity of the body to regulate itself is often underestimated when the appropriate physiological conditions are restored. In some situations, small functional interventions may have a greater impact than might initially be assumed.